COVID19: Some Quick Q&A Part III
by Raywat Deonandan, PhD
Epidemiologist & Associate Professor
University of Ottawa
(I add my credentials to these COVID-19 blog posts in case they get shared. I want readers to know that my opinion is supposedly an educated and informed one)
I have so neglected this blog of late. I had promised to add some thoughts about Sweden’s COVID-19 experiment, the science behind mask-wearing, and even strategies for re-opening schools. I still hope to get to those things. But new fatherhood has been a tad more taxing than I’d expected.
I have, though, still been doing many (too many) media engagements, talking about the latest developments in COVID-19 research. I now list those contributions in this site’s News section. Today, my significant other (known here as “The Blonde Girl”) commanded me to say no to all media requests for 24 hours. One journalist so denied commented that I was demonstrating good “husbandry”. I choose to believe it was an intentional misuse of the word, thus representing a most delicious burn that I am proud to wear openly.
So while I try to manufacture the time to craft a more thoughtful post, today you get another summary, however brief, of some of the recent questions posed to me by journalists, and the responses I offered.
Let us begin…
“I have to write a primer on contact tracing. I know the basics: an infected person is interviewed about his contacts in case the contacts may have gotten infected as a result of contact with him. What else is involved? What are the positives? The negatives?”
Contact tracing is one of the three pillars of public health infectious disease control: TTI –or, test, trace, and isolate. You can only trace if you test, because otherwise you have no one to test. And once you trace, you must test and isolate, otherwise you have accomplished nothing in terms of stemming the spread.
Every jurisdiction does tracing differently. In general, a team of tracers investigates a case (via interviewing or sometimes other tools, like tracing apps or the GPS on a phone) to determine where they have been, and hopefully with whom they’ve had contact, during the infectious period prior to detection.
The process usually involves identifying individuals who were likely contacted, and ranking those contacts has low or high risk. A low risk contact is someone you passed in the grocery store. A high risk contact is someone you had a conversation with in the elevator. Ideally, each high risk contact is tested, and if found to be positive, then is traced themselves, and so on and so on.
The process quickly becomes resource and time intensive if done properly.
“Is there a downside to contact tracing? Do any of the privacy-related concerns about it hold water?”
Not in traditional tracing. If someone asks you where you went, nothing prevents you from not giving an honest answer.
With new tracing technologies, like the tracking apps, then there is by definition some intrusion into our lives because the data is objective and passive. If privacy is the focus of your article, I would foveate on the technologies.
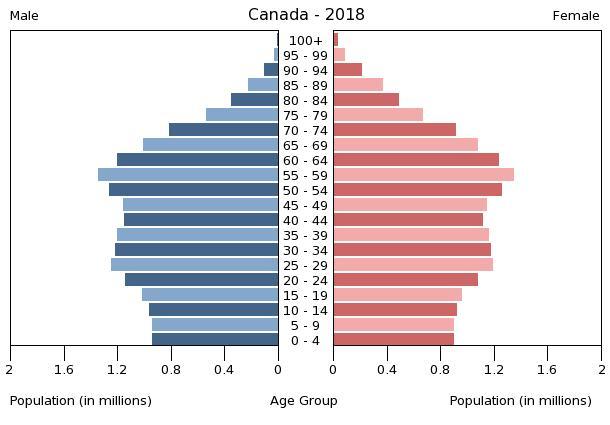
“Any idea as to why people in 50-59 year-old age group are the most infected by COVID-19 in Ontario? They’re too you young to be living in a nursing home… Is it the same in other provinces and countries?
Should Ontario have a special ad campaign/other measures targeting that age group?”
Interesting question. The age distribution of those infected is different from that of those who die (or who have serious complications)
The major risk of infection (as opposed to death) is, frankly, exposure. Who is most likely to become exposed? Those working in areas that cause the most interaction with people. In other words, people at the peak of their working lives, especially working class people, are more likely to come into contact with other people, are therefore more likely to come into contact with an infected person, and are therefore more likely to become infected themselves.
In Canada, I suspect the 50-59 age group is that population. As well, the general Canadian age distribution is fatter amongst that age group.
So there are more people in that age group in the general population, so it’s not surprising that the same distribution is represented in the COVID patient database.

This is distinct from the age-specific risk of becoming infected. These data (the COVID age distribution, do not show the RISK of each age group becoming infected. That’s a common misunderstanding of the data. A distribution is not the same as an age-specific incidence rate.
“Why is BC doing so much better than Ontario?”
There are at least three reasons: luck, timing, and leadership. In terms of luck, BC has a smaller population, lesser urban concentration, distance from the hotspots of New York and Europe, and a more disperse population across a very large province.
In terms of timing, BC had their March break later than Ontario and was able to learn from our mistake. That’s where the good decision making comes in, as the best decisions led to prompt action, hence timing.
Unlike Ontario, BC worked fast to “nationalize” its long term care centres (LTCs), assuring workers high wages as a disincentive for having to work in several centres (which was a major source of infection in Ontario). Those staff were also provided PPE (personal protective equipment) earlier than Ontario; in fact, distribution of PPE was organized centrally by the province, not relegated to each institution to manage.
BC started its testing and tracing program in earnest earlier than Ontario. This was the result of strong central leadership by experts in public health. This leadership also manifested in how data was collected and shared, and how the full capacity of the province –labs, academics, other specialists– were mobilized toward a single purpose. These are things that Ontario continues to struggle with.
I will add, though, that I think it’s largely a mistake to compare regions in this way. There is so much heterogeneity in population dynamics, geography, infrastructure and the factors you can never quantify, like luck, that often the exercise creates more uncertainties than it addressed.
“What do you think about travel bubbles? (The idea that different countries or provinces or states can allow unimpeded travel between the two, once their COVID situation is better controlled.)
So much to unpack here. First, there is heterogeneity: in case loads, public health systems, leadership, and social compliance with public health rules. Australia and New Zealand are natural bubbles. They are culturally similar, have low case counts, and are well separated from other countries.
This leads to the natural second factor, which is the most important: trust. Do you trust the other jurisdiction to be as stringent and as transparent with their public health policies? Some of this varies with the ways that each area collects, computes, and shares cases. Without transparency there can be no trust.
How will travel take place? If it’s a flight, then there can be no intervening airport in a third country. Where will the airline originate? If Australia and New Zealand travellers solely use Quantas, that’s one thing. But if they use Emirates Air, then there is lesser national control over the plane’s hygiene and its practices when not in the travel bubble space.
One of the biggest questions I have is what happens when someone tests positive? There are initiatives to test the bubble idea wherein travelers are isolated for 14 days, and tested before boarding a plane. I think they should be tested again upon landing to minimize the chance of false negatives. But my question is, what do you do when someone tests positive? Do you quarantine the whole plane? The whole airport? Plans must be made for such contingencies.
Can you comment on Dr Alberto Zangrillo’s claim that the virus is “losing potency“?
(a) First, beware of science by press release or YouTube video. If there are actual data to be presented, present them and let the scientific community render peer review. To my knowledge, no such data have yet been presented.
(b) Second, while it is possible (and inevitable in the very long run) that this virus will mutate toward non-lethality, it shows no signs of doing so yet anywhere else in the world. So any such claim needs some strong evidence.
(c) Beware expertise creep. Dr Zangrillo is not a virologist, geneticist or epidemiologist. Remember when everyone was alarmed that people in Asia were being reinfected by the virus? Only the epidemiologists were saying that it was likely a testing failure; and we were right. Similarly, Zangrillo has observed reduced viral load in his swabs of infected patients and has jumped to the conclusion that the virus has mutated. It is more likely that as the first wave wanes, he is increasingly testing lesser symptomatic people with lesser viral load. It’s possibly an epidemiological testing bias.
So I cannot stress this enough… wait for proper scientists to render judgement; do not let media do so.
From a reader, not a journalist: “Is it possible a larger portion of the population has already been infected than we’re aware of?”
Your question is a very common one. And the answer is both yes and no. COVID has been in North America from at least January, possibly even late December (flights from China being as frequent as they are). So it is unavoidable that more of us have been exposed than what is commonly thought.
This is not in and of itself truly controversial. It’s the extent of the exposure that is debatable. Those arguing that this disease is not that serious claim that many (most?) already have had it and don’t know, therefore the IFR (infection fatality rate) is very low and we are close to herd immunity.
However, now that we are doing seroprevalence studies (tests of blood samples to see the extent of previous infection), the data does not support that conclusion. In New York state, about 15% have been exposed (which is high). In Stockholm (another place with heightened infection) it’s more like 7%. In Canada, we have started the process but don’t know. But Angus Reid did a qualitative poll to measure COVID-like symptoms and estimated a prevalence of under 5%, I believe. Most experts think Canada’s exposure is 2-7%, including the mild and asymptomatic cases.
You might recall that herd immunity for this disease probably kicks in at 40-70% (which is also debatable for other reasons). So we’re not near that yet. And the IFR estimates based on these new data around 0.6-1.2% –which is high compared to the worst season of the flu, which is 0.12%
In short: while absolutely more people have had it than we know about, that doesn’t mean this is not a very serious disease and that our population is not mostly susceptible.
—
Well, I’m exhausted. A newborn baby will do that. Sorry I can’t write more today. But I promise I will do more very soon.

{kind=link}